

Cholangio 101
Patient to Patient – Caregiver to Caregiver
Connecting and sharing Knowledge, Experiences and Wisdoms

 Hi my name is Nicole Griffith and I am a supporter, advocate and caregiver for my father.
Hi my name is Nicole Griffith and I am a supporter, advocate and caregiver for my father.Treat the immune not the Cancer
How to reactive the immune system to defeat the Cancer

Ipi/Nivo is treating the immune not the Cancer itself with it’s two pronged attack
How Does Ipilimumab (Yervoy) Work?
CTLA-4 is a protein that sits on the surface of a T Cell, it’s job is to deactivate a T cell attack on healthy cells …
Ipilimumab blocks the CTLA-4 from deactivating the attack and allows thean increased immune response.
How Does Nivolumab (Opdivo)? Work?
PD-1 is a protein that sits on the surface of a T Cell, it’s job is to act as a fail safe when engaging with the suspect cell – If it detects a corresponding PD-L1 protein that sit on t he surface of health cells they bind and deactivate the T Cell attack
Tumor affected cells have learnt to express this PD-L1 protein on their surface when they detect an attack, thereby tricking the T Cells and avoiding an attack.
Nivolumab (Opdivo)blocks the PD-1 from detecting the PD-L1 thus allowing the attack to continue
Panel Discussion
Explains rationale and Benefit over Chemotherapy treatment with the new direction in cancer treatments of “Treat the Immune not the Cancer itself, this is changing survival in cancer.
Good explanation Videos
PD-1 PD -L1 Pathway + Car-T cell
Jim Allison
Nobel Prize winner
Immunotherapy – CTLA-4 break through
Cholangio 101
Important











Pdf Overview
Pronunciation
Cholangiocarcinoma is the clinical name for Bile Duct Cancer. The easiest way to pronounce this name is to first break it in half, ie: Cholangio + carcinoma
Chol – angio + car -cinoma
Meaning
“Chol’e means bile: angio means vessel:” Bile Duct
Carcinoma means a type of Cancer
A cancer originating within the Bile Ducts
Cholangiocarcinoma Abbreviations: CC 0r CCA
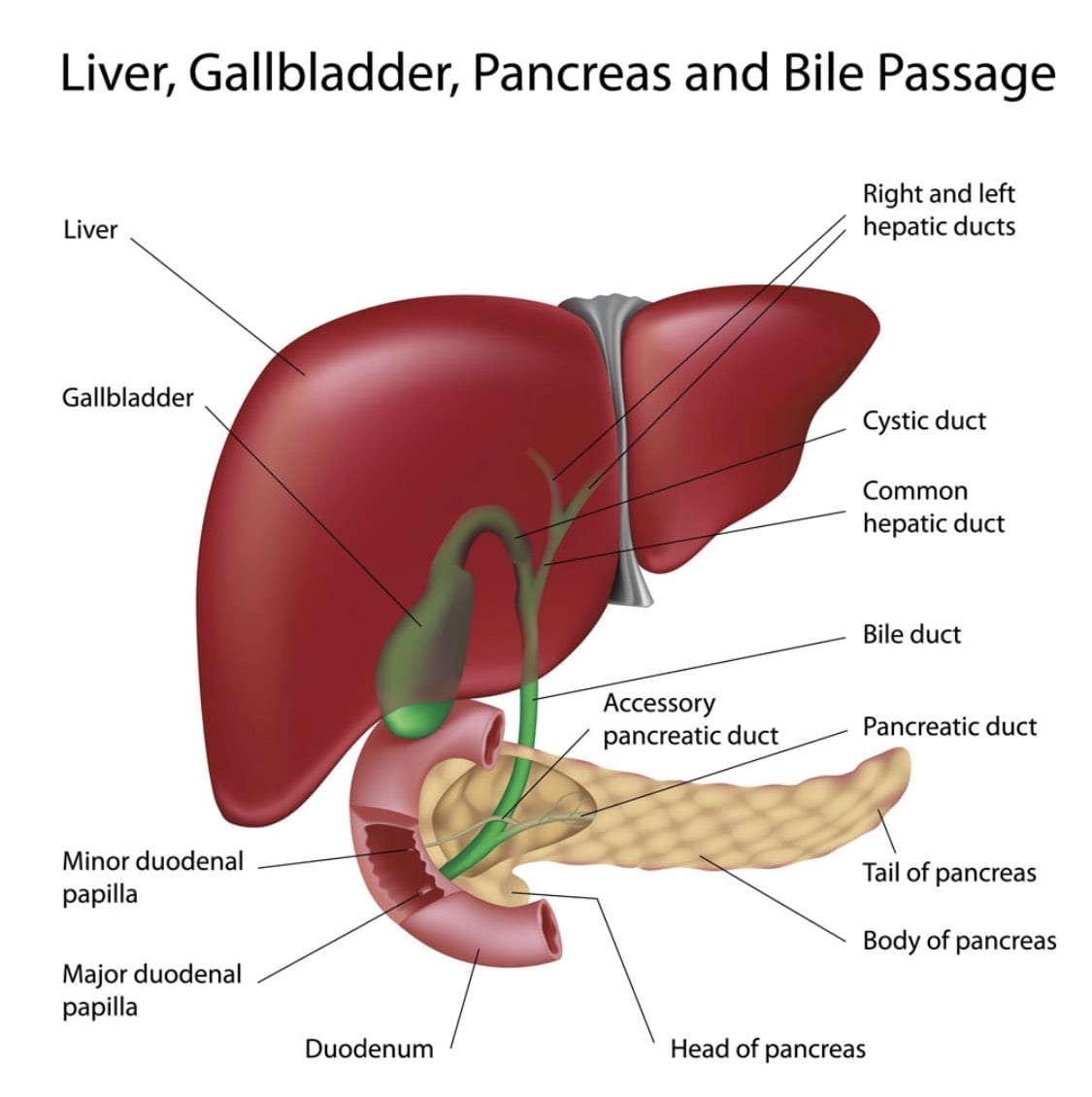
Cholangiocarcinoma originates in the thin Bile Duct tube which is about 125 -150 mm long, extending from the liver to the small intestine (Duodenum). The bile ducts function is to move a fluid called bile from the liver and gallbladder to the small intestine, where it helps digest the fats in food.
Different parts of the bile duct system have different names. In the liver it begins as many tiny tubes (ductules) where bile collects from the liver cells. The ductules come together to form small ducts, which then merge into larger ducts and eventually the left and right hepatic ducts. The ducts within the liver are called Intrahepatic bile ducts. These are the ducts that exit from the liver and join together and form the common hepatic duct at the hilum.
About one-third of the way along the length of the bile duct, the gallbladder (an organ that stores bile) attaches by a small duct called the cystic duct. The combined duct is called the common bile duct. The common bile duct passes through part of the pancreas before it empties into the first part of the small intestine (the duodenum), next to where the pancreatic duct also enters the small Duodenum.
Tumours can develop in any part of the bile duct and, based on their location, are classified into 3 types. (Primary)
Intrahepatic cholangiocarcinoma
Perihilar cholangiocarcinoma
Distal cholangiocarcinoma.
Cancers in these different areas may cause different symptoms.
Cholangiocarcinoma can also be divided into types based on how the cancer cells look under the microscope. More than 95% of bile duct cancers are carcinomas and most are adenocarcinomas. Adenocarcinomas are cancers of glandular cells that can develop in several organs of the body. Bile duct adenocarcinomas develop from the mucous glands that line the inside of the duct. Cholangiocarcinoma is another name for a bile duct carcinoma.
Content reinterpreted from CCF
The Cholangiocarcinoma Foundation
Adenocarcinomas are also prominent in
- Lung cancer: Non-small cell lung cancer accounts for 80 percent of lung cancers, and adenocarcinoma is the most common type.
- Prostate cancer: Cancer that forms in the prostate gland is typically an adenocarcinoma, which accounts for 99 percent of all prostate cancers.
- Pancreatic cancer: Exocrine pancreatic cancer tumors are called adenocarcinomas. They form in the pancreas ducts.
- Esophageal cancer: Cancer that forms in the glandular cells of the esophagus is known as adenocarcinoma. This is the most common type of esophageal cancer.
- Colorectal cancer: Cancer that develops in the intestinal gland cells that line the inside of the colon and/or rectum is an adenocarcinoma. It makes up 95 percent of colon and rectal cancers.
- Adenocarcinoma may also develop elsewhere in the body.
Primary Location defines your CC type
Every Tumour has a birth place – a beginning point
This origin location, referred to as your Primary Tumour and defines your diagnosis.
There are two general primary locations
- Intrahepatic CC – Primary within the bile ducts and within the Liver
- Extrahepatic CC – Primary within the bile ducts outside the Liver
Extrahepatic Primary’s are further defined as per the diagram below.
- Perihilar Extrahepatic Primary is located in the Hilum/Common Hepatic Duct region – just under the liver adjacent to the Gallbladder
- Distal Extrahepatic Primary is located in the Common Bile Duct – just below the junction to the gallbladder and extends down to the Duodenum

There are other more outdated names such as Hilar or Klatskin Tumours which means Perihilar
Surgery if possible
- Surgery is a potential Curative intervention
- Only a very small percentage qualify for surgery, due to most diagnosis are late stage and metastatic.
- Curative Surgery Outcomes are also very small with most patients relapse.
Chemotherapy a Management tool
- Chemotherapy is a management tool
- Chemotherapy is not a curative treatment.
- Primary objective to slow or stop progression
- Some patients see overall regression
- Some Patients see all visible cancer activity eliminated – NED (No Evidence of Disease.
- Cholangiocarcinoma’s First line Chemotherapy Treatment is Gemcitabine and Cisplatin (Gem/Cis)
- Typical First line treatment duration is 6 months
- Treatment cycles 2 week on – 1 week off
- Scans to measure treatment is 9 weekly or 12 Weekly dependant on aggression.
- Variations: There are many more combinations including combining with Immunotherapy drugs. The basic idea behind this is for the chemotherapy agent to first do a general knock down to weaken all cells and then introduce the immunotherapy drug to have a greater chance of success.
Symptoms appear late
Sudden onset of abdominal pain, Fatigue, then jaundice, and weight loss. These symptoms are similar to many other ailments in the beginning and therefore often dismissed.
There is no current early detection method for CCA.
It is unfortunate that most patients will feel no ill effects until the cancer is very advanced. This is one of Cholangiocarcinoma’s biggest threats, and contributes to many being excluded from a potentially curative surgery.
Most common Symptoms
- Chills
- Clay-colored stools
- Fever
- Itching
- Loss of appetite
- Weight loss
- Pain in the upper right abdomen that may radiate to the back
- Yellowing of the skin
Staging
Staging is a way of describing a cancer, such as where it is located, if or where it has spread, and if it is affecting the functions of other organs in the body. Doctors use diagnostic tests to determine the cancer’s stage, so staging may not be complete until all the tests are finished. Knowing the stage helps the doctor to decide what kind of treatment is best and can help predict a patient’s prognosis (chance of recovery). There are different stage descriptions for different types of cancer.
One tool that doctors use to describe the stage is the TNM system. This system uses three criteria to judge the stage of the cancer: the tumor itself, the lymph nodes around the tumor, and if the tumor has spread to the rest of the body. The results are combined to determine the stage of cancer for each person. There are five stages: stage 0 (zero) and stages I through IV (one through four). The stage provides a common way of describing the cancer so doctors can work together to plan the best treatments.
TNM is an abbreviation for tumor (T), node (N), and metastasis (M). Doctors look at these three factors to determine the stage of cancer:
How large is the primary tumor and where is it located? (Tumor, T)
Has the tumor spread to the lymph nodes? (Node, N)
Has the cancer metastasized (spread) to other parts of the body? (Metastasis, M)
Intrahepatic Cholangiocarcinoma (cancer that occurs in the bile duct within the liver) is staged using the same system as liver cancer. The staging of both Intrahepatic and Extrahepatic Cholangiocarcinoma is below.
Stage 0 to 4
Basic Staging Descriptions
- Grade 0: The cancer is only growing in the innermost layer of the bile duct and has not spread to lymph nodes or distant sites.
- Grade 1: The cancer has grown into deeper layers of the bile duct wall but it has not grown all the way through the wall. It has not spread to lymph nodes or distant sites.
- Grade 2: The cancer is either a single tumor that has grown into a blood vessel (T2a) or there are multiple tumors (T2b). The cancer has not grown into any nearby organs or structures. It has not spread to nearby lymph nodes (N0) or distant sites (M0).
- Grade 3: The cancer has grown into nearby structures such as the duodenum (first part of the small intestine), colon, stomach, abdominal wall, diaphragm, or lymph nodes around the portal vein. It has not spread to nearby lymph nodes or distant sites.
- Grade 4: The cancer has spread (metastasised) to other organs away from the original primary site.
Statistics
We are currently updating the statistics info for Newly Diagnosed Patients per year
This page will be updated soon.
Australia: Sub 1,000 – est 900 (to be confirmed)
USA-North America : Sub 10,000 – est 9,000 (to be confirmed)
UK and Europe: (to be confirmed)
Overall Average Survival Period = 6.8 months
Cholangiocarcinoma Foundation
www.cholangiocarcinoma.org
The incidence and mortality of Cholangiocarcinoma in North America and Europe has increased dramatically in the past few decades.In the U.S., there are now between 5,000 and 10,000 new cases diagnosed each year.
Rates are highest among Hispanics and Asians, and men appear to have a slightly greater mortality from the disease than women.
The highest incidence rates are in Eastern and South-Eastern Asia, with a peak in Thailand.
The prognosis for bile duct cancer
5 Year Survival Rates
Seers all stages
- Intrahepatic: 8%
- Extrahepatic 10%
- Metastatic – Intra or Extra: 1 %
See Source Link for all variations
Seers
The American Cancer Society relies on information from the Surveillance, Epidemiology, and End Results (SEER) database, maintained by the National Cancer Institute (NCI), to provide survival statistics for different types of cancer.
Good resource for terminologies
What is Primary Cancer?
This is the original tumour location. A tumour in the bile duct is called a Cholangiocarcinoma, if it spreads (Metastasises) to other parts of the body ie. Lungs, it is still Cholangiocarcinoma, not lung cancer etc.
What is Metastasis?
When the cancer spreads to other locations away from its primary tumour location ie. Lungs, Liver etc.
What is a Mutation?
Any change in the DNA sequence of a cell. Mutations may be caused by mistakes during cell division, or they may be caused by exposure to DNA-damaging agents in the environment.
What are the Curative Options?
- Surgical operations are the only known Curative action, but stats are very poor
- More recently immunotherapy has been seen as a curative option
What are the Surgery Procedures?
- ECRP: Surgical, typically investigative same day procedure via the mouth
- Whipple: Surgical, a significant operation typically removing all or part of multiple sites such as gallbladder, head of the pancreas and stomach
- Resection: Surgical, typically refers to Intrahepatic patients, removing a portion of the liver and gallbladder. This can also refer to removing a section of the bile duct for Extrahepatic patients which often include the gallbladder.
What is Chemotherapy?
- A drug that is infused or oral
- Typically the first line action is Gem/Cis – Gemcitabine & Cisplatin
- Chemotherapy is not regarded as curative, but the best management tool available
- Chemotherapy as an infusion process carried out in the Chemo wards of most hospitals, typically this will take 3 – 5 hours. Some Chemotherapy options such as Capecitabine are taken orally
Most treatment programs are 3 to 6 months in length and can be repeated several times.
What is the CA 19- 9 Marker?
A measure in a blood test (carbohydrate antigen) – a tumor marker that is observed in elevated serum concentration with metastatic GI cancers. This is not always an accurate measurement.
What are Trials?
There are many trials coming available in both immunotherapy and combination immunotherapy and Chemotherapy. Most patients embrace trials as an opportunity to move forward.
What is Immunology?
Immunology is a fast evolving knowledge pool of using the body’s immune system to defeat cancer. Immunotherapy is the specifically designed options derived from the immunology pool that are applied to the patient. This is worth reading up about …[continue]






")